Differential Diagnosis: "Climber's Elbow"
So you’ve got tendonitis, climber’s elbow, golfer’s elbow, or medial epicondylitis and you did your work searching the internet to fix yourself. You’ve took time off, stretched the heck out of it, did eccentrics, maybe even found some handy ways to use a lacrosse ball to “break up scar tissue.” Unfortunately, you’re still having pain.
Let’s talk about how to differentiate what else could be going on. . .

Epicondylitis:
The epicondyle is the sticky outie bit on either side of elbow, and is part of the bone named the humerus.
Itis means inflammation.
Usually it is the tendon (the tissue that attaches your muscle to the epicondyle) that gets inflamed so it is called Epicondylitis. Practioners will also use the term Epicondylosis to describe the same thing if it has been a more chronic issue.
DIAGNOSING TRUE TENDONITIS AT THE MEDIAL EPICONDYLE
Three Tests:
1. Resisted wrist flexion **no matter what position the wrist or elbow is in.
2. Stretching the wrist flexors.
3. Pressing/palpating the tendon.
Also note that pronator teres could be the culprit and you would use the same methodology above to differentiate that tendon from the wrist flexors (resisted pronation, stretched supination, and palpation).
If you don’t have pain with ALL THREE of these tests, then you don’t have tendon inflammation. HOW EASY IS THAT?!
So I don’t have tendonitis. What else could it be?
Joint Dysfunction:
Joints are the areas where two or more bones come together and allow for movement.
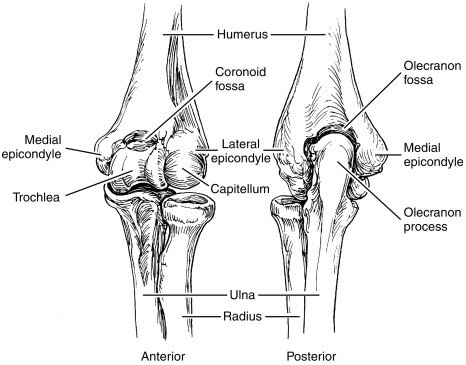
The photograph on the right is helpful to see the three joints of the elbow.
1. Humero-ulnar joint- The olecranon process of the ulna gliding with the olecranon fossa of the humerus.
2. Humero-radial joint- The concave radial head spinning and gliding with the capitellum of the humerus.
3. Radio-ulnar joint- The convex side of the radius rolling on the ulna.
The joint can become painful if it is hypermobile (moving too much) or hypomobile (moving too little) in a certain direction which causes stress on surrounding tissues including ligaments, the capsule that surrounds the joint, or the cartilage between the joints.
As you can see, part of the humero-ulnar joint is located at the medial epicondyle so for this post lets focus on that joint.
DIAGNOSING JOINT DYSFUNCTION
1. Fully flex your elbow. Does this reproduce your medial elbow pain? YES go to step 2. NO move on to another diagnosis :)
2. Try this elbow distraction and see if it helps: https://www.youtube.com/watch?v=MPXjtixjWoU
3. If the joint distraction helps then you may want to start using that to loosen up prior to your normal training routine.
This is what we call a “quick test” and is not a thorough assessment of the biomechanics of the elbow entirely. It is a cool initial guide towards differentiating compressive or positional pain vs. the tendon pain tests we discussed above.
If you suspect a joint dysfunction such as a fracture, bone spur, arthritis etc have it further evaluated by a PT for more guidance!


Nerve Referral:
Let us just start by saying that the nervous system is SO COOL and issues with it are SO COMMON.
There are two ways of thinking about the nerves to the arms.
Proximally- the nerve roots that exit from your cervical spine
The letter and number correspond to which vertebra they exit between for example C4 is the root between the 4th and 5th cervical vertebra.
These roots allow for both movement and sensation along your arm.
If the root itself get irritated at the level of the neck you can have pain, among other symptoms, in the corresponding region down your arm like the photo to the left.
Distally- peripheral nerves that run down your arm
Once the nerve roots exit the neck they branch out into what we call peripheral nerves.
The two that travel near your medial elbow are the median and the ulnar nerves.
DIAGNOSING RADICULOPATHY/ NEUROPATHY
Cervical Range of motion: Pain in the elbow is reproduced when moving the neck into different positions causing the nerve root to get pinched or stretched
Loss of strength, loss or changes in sensation (numb, tingling, cold, hot) or decreased/ increased reflexes.
Pain is reproduced by performing nerve tension tests for median or ulnar nerve.
Pain is reproduced by “strumming” the nerve.
If you suspect you have nerve involvement it is useful to differentiate if it is proximal vs. peripheral because that can guide your treatment.
As you can see there are many things that could be causing medial sided elbow pain other than the tendon. And of course there are even more not included here such as ligament, bursa, fascia among others.
Having a proper diagnosis can make all the difference in what to do for treatment, significantly affecting outcomes. Reach out or book an appointment below if you have more questions or need help!